
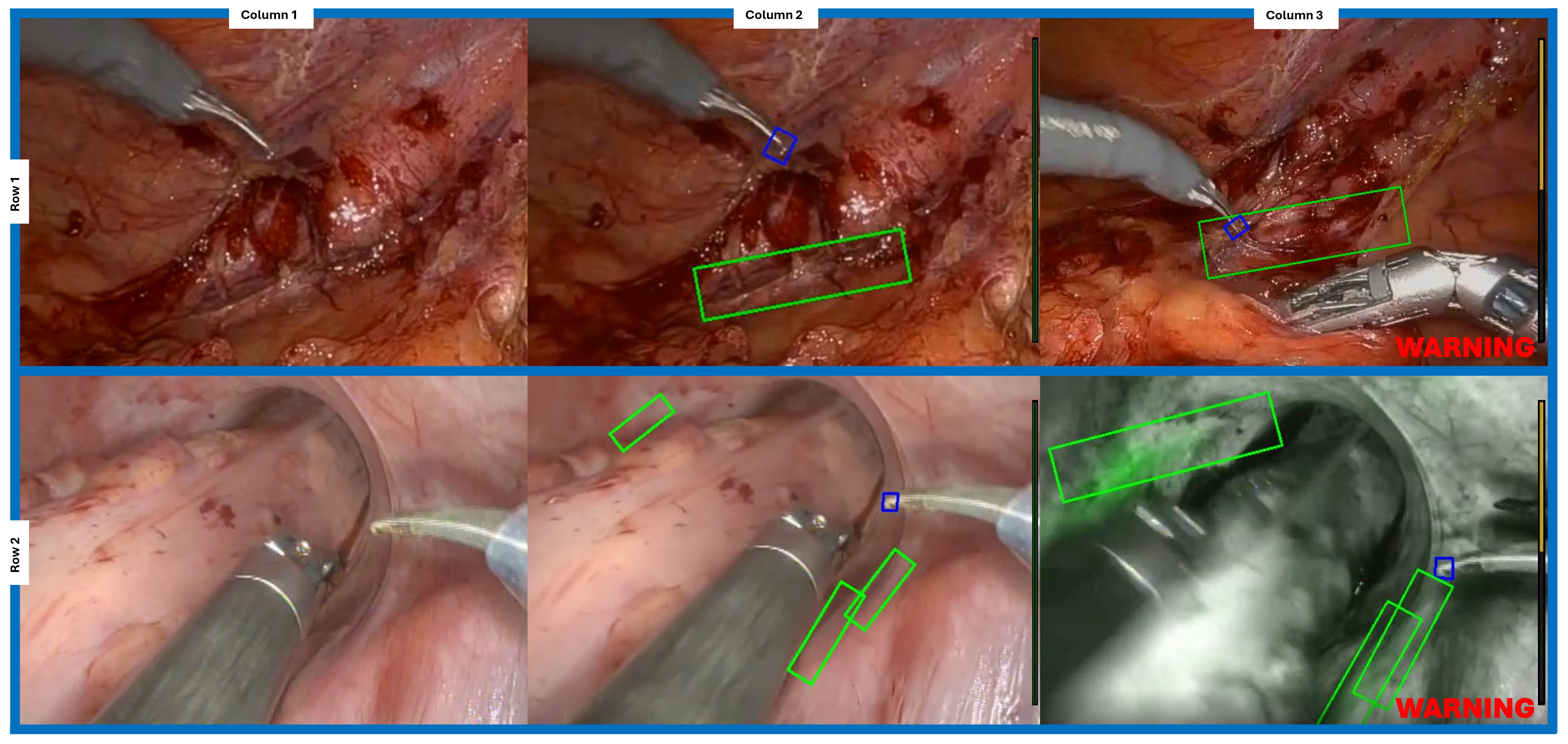
 Figure I: Row 1 shows operative field during IMA dissection. Row 2 shows operative field during rectal dissection. Column 1 shows original video frame. Column 2 shows AI-automated object identification for the ureters (green box) and instrument tips (blue box) taken in real-time during live video. Column 3 shows the warning signals activated during proximity of instrument tips to the ureter with and without Firefly mode.
Figure I: Row 1 shows operative field during IMA dissection. Row 2 shows operative field during rectal dissection. Column 1 shows original video frame. Column 2 shows AI-automated object identification for the ureters (green box) and instrument tips (blue box) taken in real-time during live video. Column 3 shows the warning signals activated during proximity of instrument tips to the ureter with and without Firefly mode.